

The leading Endocrinology EMR Software from a trusted name in healthcare — 1st Providers Choice
IMS for Endocrinology – Our extensive knowledge of the diabetology and endocrinology fields allow us to offer a comprehensive EMR software installation package for endocrinology customers and diabetic patients. This IMS-integrated endocrinology EMR and Practice Management suite is customized to the endocrinology profession to provide full electronic practice management.
Endocrinology EMR Software solution offers a solid set of features to enhance patient care and boost profitability. Our years of experience working with endocrinologists has given us the tools and experience to implement highly successful EMR software for diabetic patients.
The IMS integrated endocrinology EHR and Practice Management suite is tailored to endocrinologists’ needs throughout the application, from documentation templates and content to practice management.
Learn more about the benefits of EMR software.
Black Book 2025 Award Winner
Voted One of Black Book Market Research’s Top Endocrinology EMR for 2025.
Our monthly IT expenses were reduced over 87% after implementing IMS – a huge savings for our company.
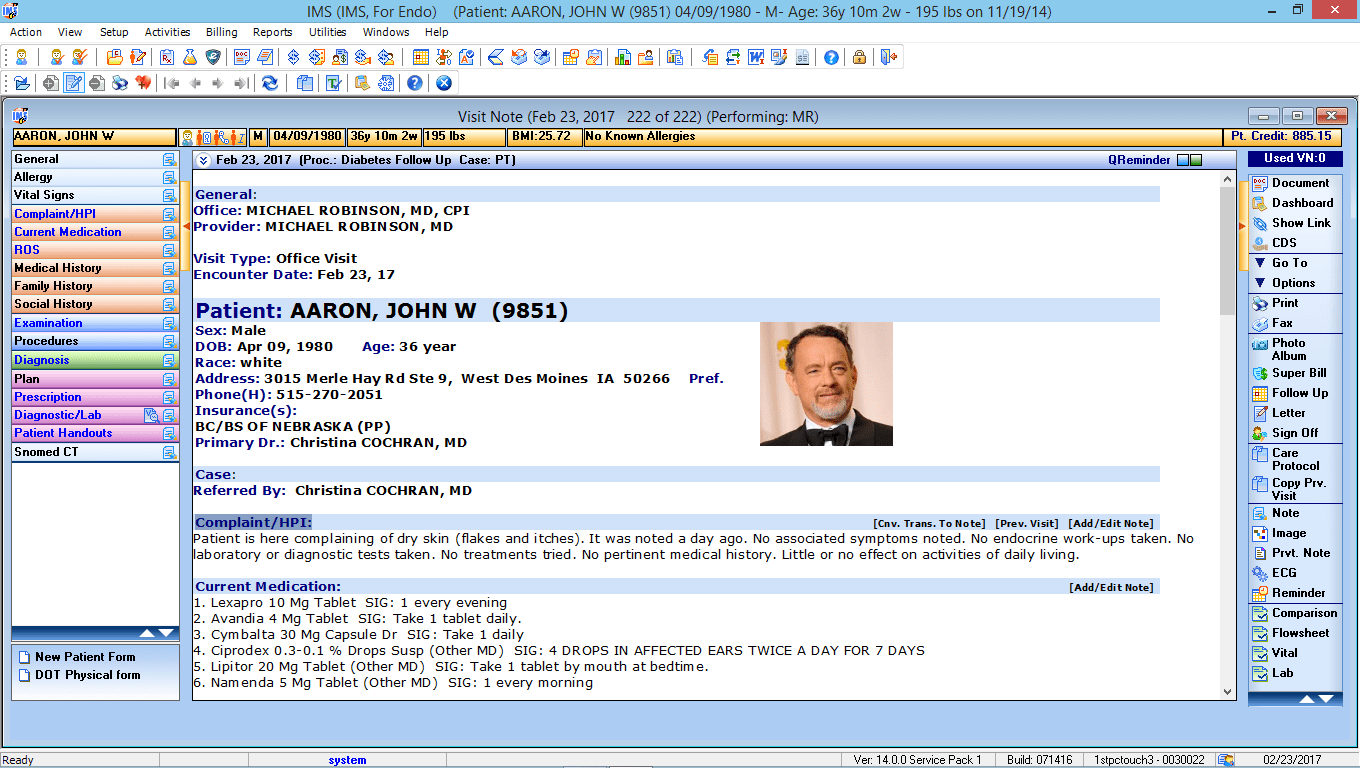
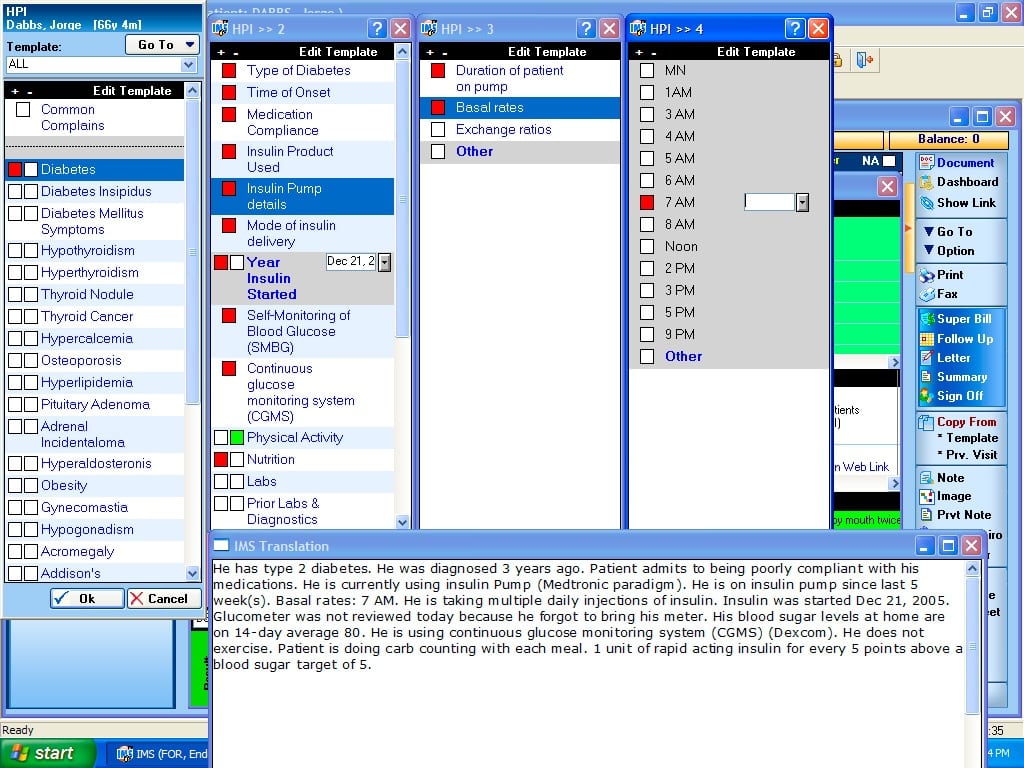
EMR & Patient Visit Notes
IMS’ image-based Endocrinology EMR software allows physicians to include drawings with their documentation and make notes on imaging results and other patient-related images.
Benefits
- Provide more detailed findings
- Streamline the documentation process
- Improve workflow
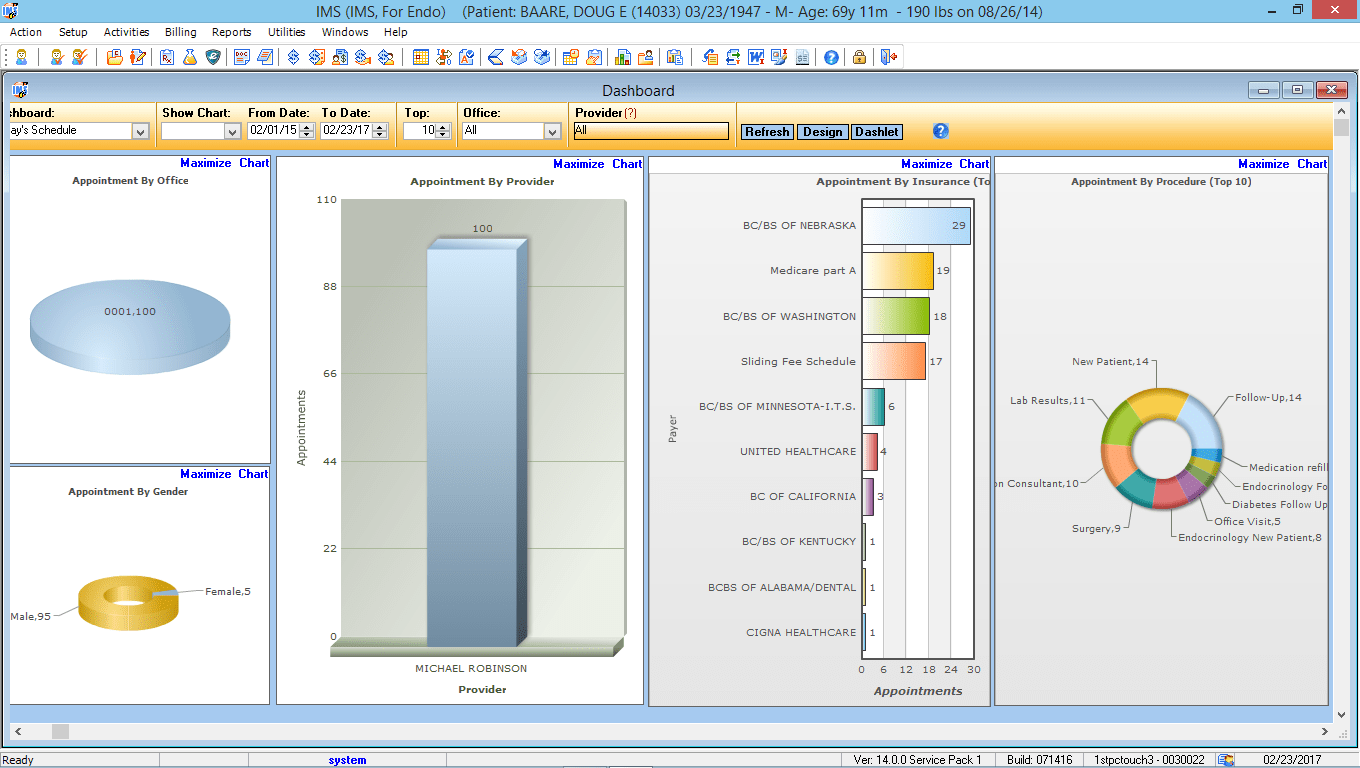
Patient Dashboard
IMS’ Patient Dashboard offers a summary of all patient information stored within the EMR. Here, endocrinology specialists can view data such as demographics, problems, medications, and more.
Benefits
- Get important information at-a-glance
- Better understand your patients’ health
- Make more informed decisions

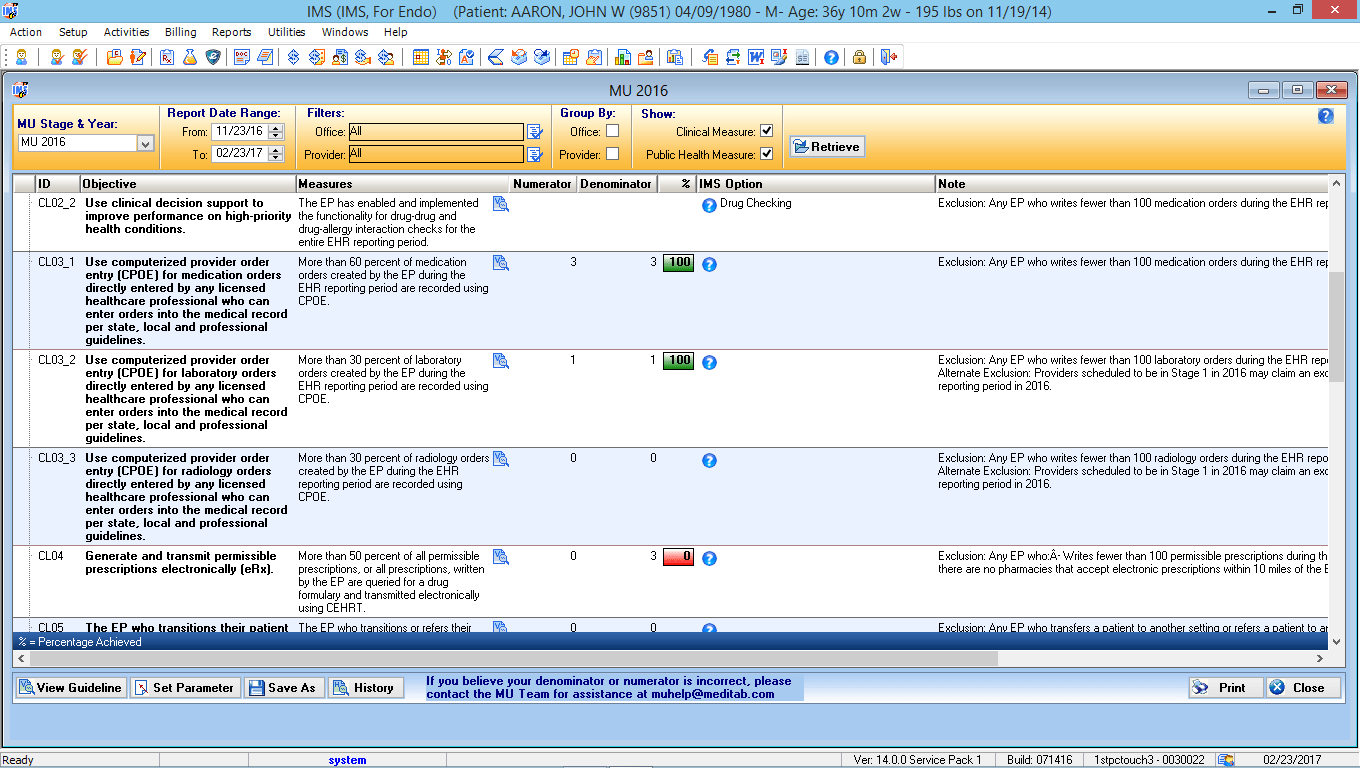
Meaningful Use Dashboard
Manage and track your Meaningful Use progress with our interactive Meaningful Use Reporting module. Gather real-time indicators of current Meaningful Use levels, view percentages of compliancy, and more.
Benefits
- Ensure attestation objectives are met
- Meet Meaningful Use requirements
- Monitor problem areas daily
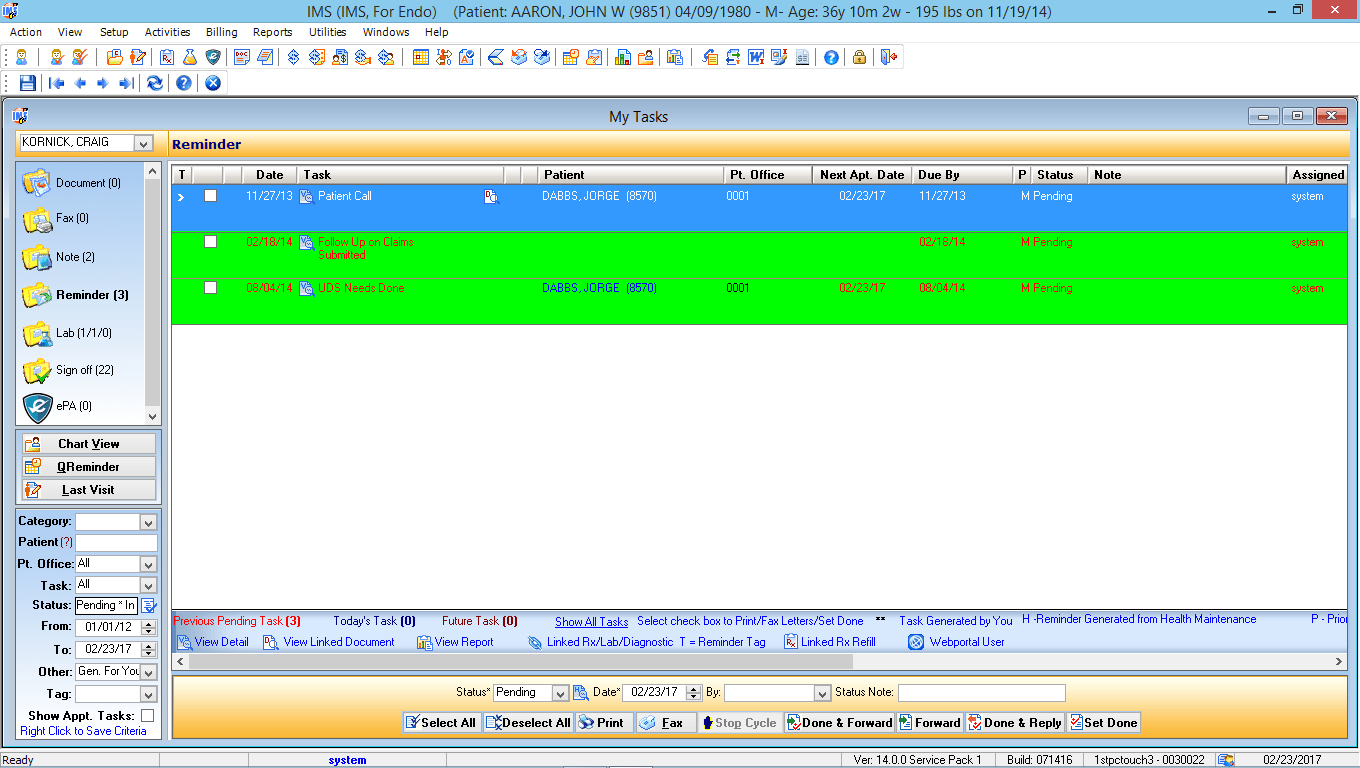
Provider Task List
IMS’ Personal My Tasks List alerts doctors and staff about unfinished tasks that can affect patient care. It includes notifications regarding lab results, unsigned visit notes, and more.
Benefits
- Track patient care from start to finish
- Improve intra-office communication
- Achieve maximum productivity
- Improve office workflow
Alerts and Reminders
The Endocrinology EMR Software is fully integrated modules within IMS alert doctors and staff of important tasks related to patient care. It includes follow-up appointments, specialist referrals, medication management, and many more.
Benefits
- Improve preventive care efforts
- Increase practice productivity
- Provide better patient care
- Customize alerts to your specialty

Attorney Portal
Provide attorneys with access to necessary medical documentation, such as itemized bills, reports, and disability slips, for their ongoing personal injury and Workers’ Compensation cases.
Benefits
- Eliminate paper-based processes
- Better serve your users
- Increase staff productivity
- Meet HIPAA standards
Doctor/Provider Portal
With IMS’ Endocrinology provider portal, Endocrinology specialists can use self-service tools to access messages, communicate with patients, and more. The portal also ties into the use of our telemedicine system.
Benefits
- Meet Meaningful Use requirements
- Manage patient accounts online
- Improve care coordination
- Streamline workflow
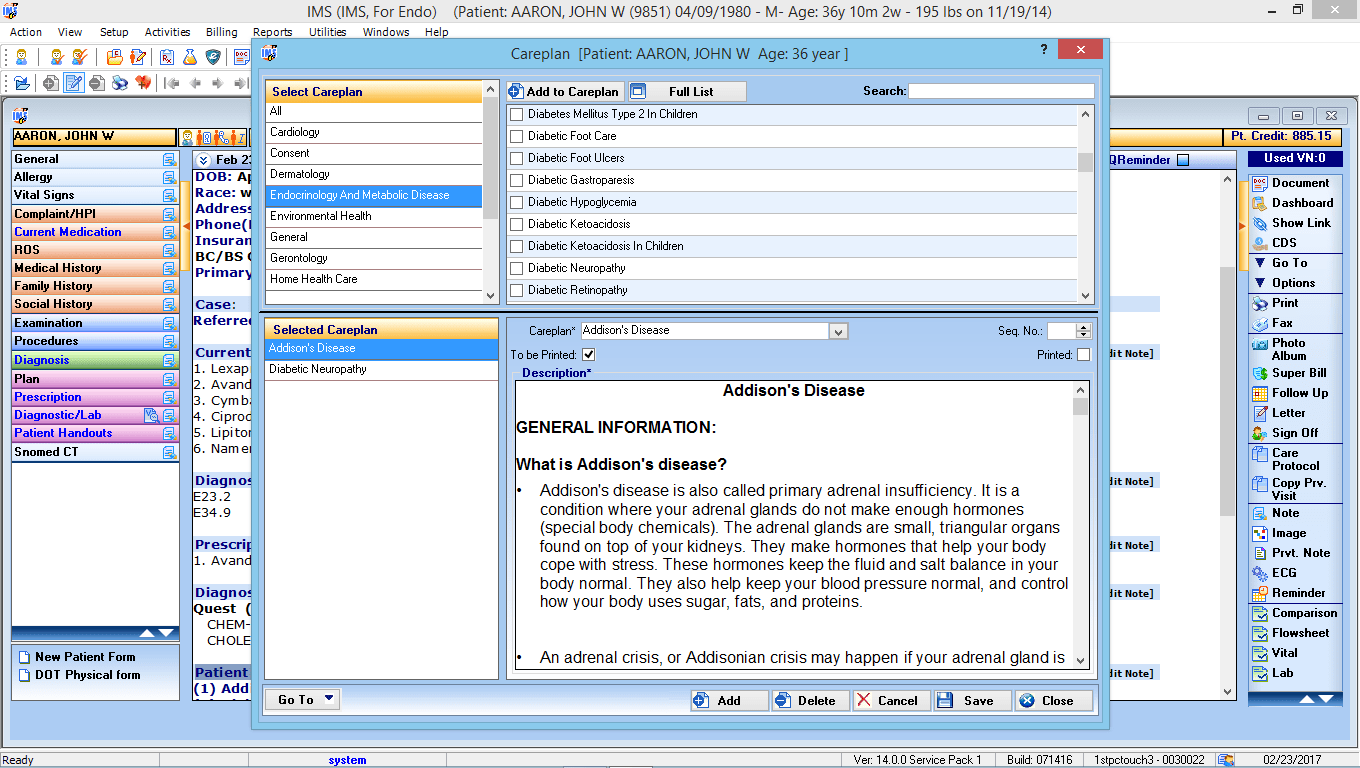
Care Plan
Come up with a care plan for your Endocrinology patients, and IMS EMR will generate a patient education handout based on the selected diagnosis and condition.
Benefits
- Increase patient engagement
- Improve quality of care
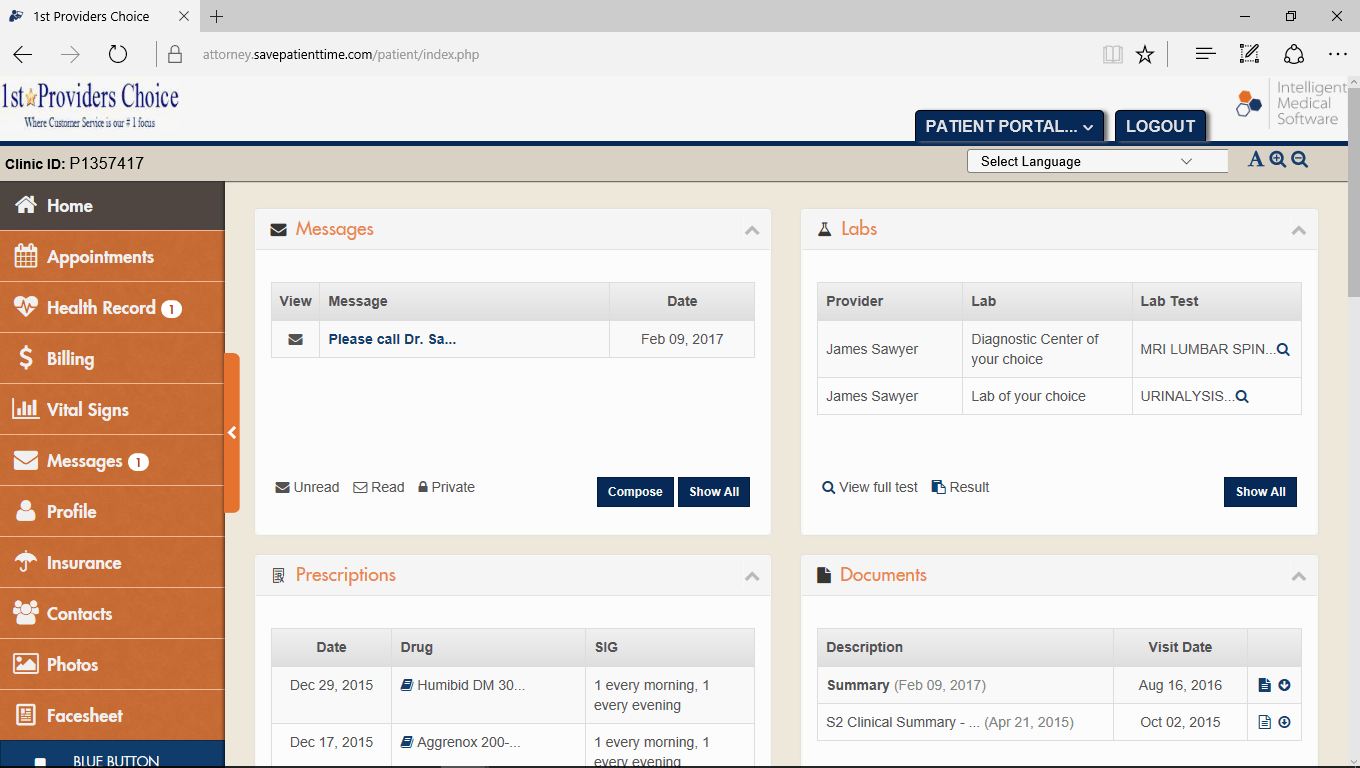
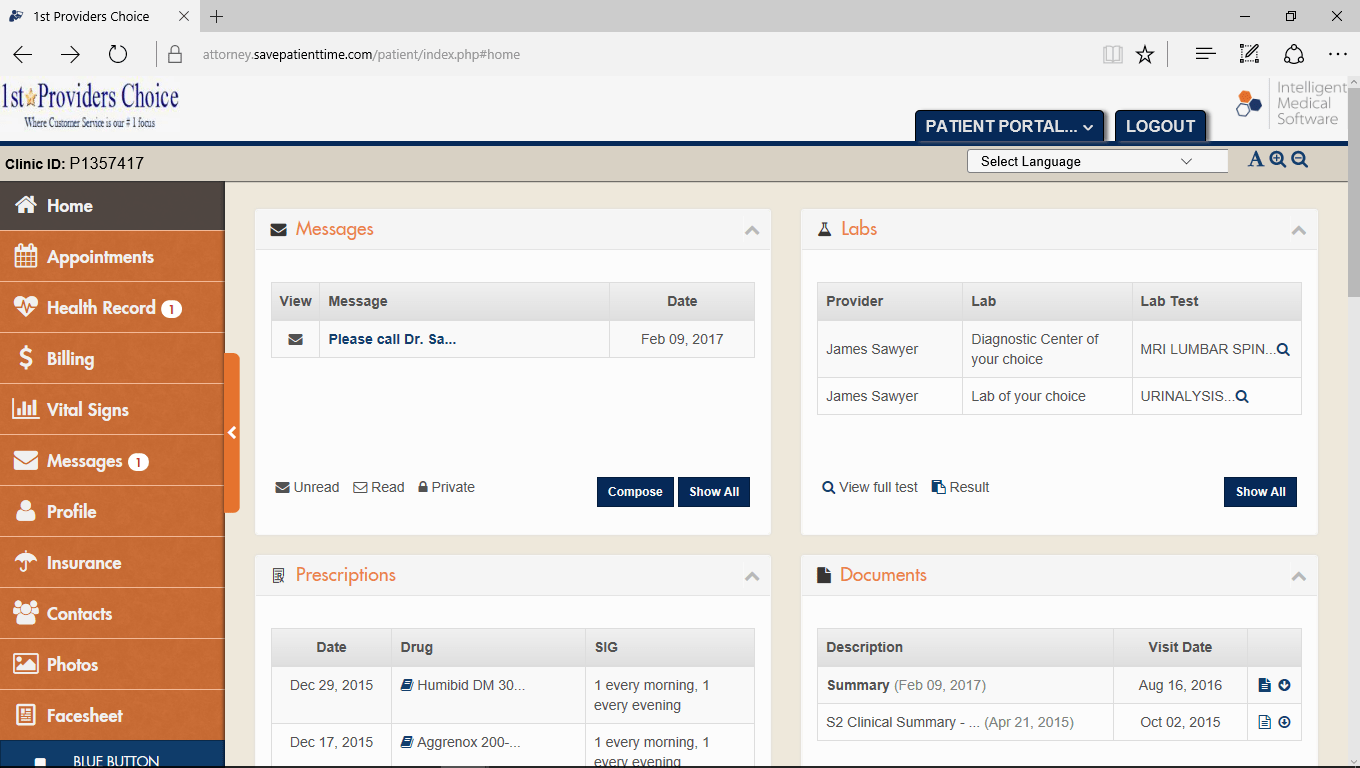
Patient Portal
Involve patients in their health care by offering access to an online patient portal. With our portal, your patients will be able to view visit summaries and test results, request medication refills, and much more.
Benefits
- Streamline administrative processes
- Reduce workload
- Increase patient satisfaction
- Meet Meaningful Use requirements

Voice Recognition
With speeds of up to 160 words per minute and accuracy in the 98 to 99 percentile range, using voice recognition software for medical documentation has never been easier.
Benefits
- Reduce documentation time
- See fewer errors
- Improve the quality of care
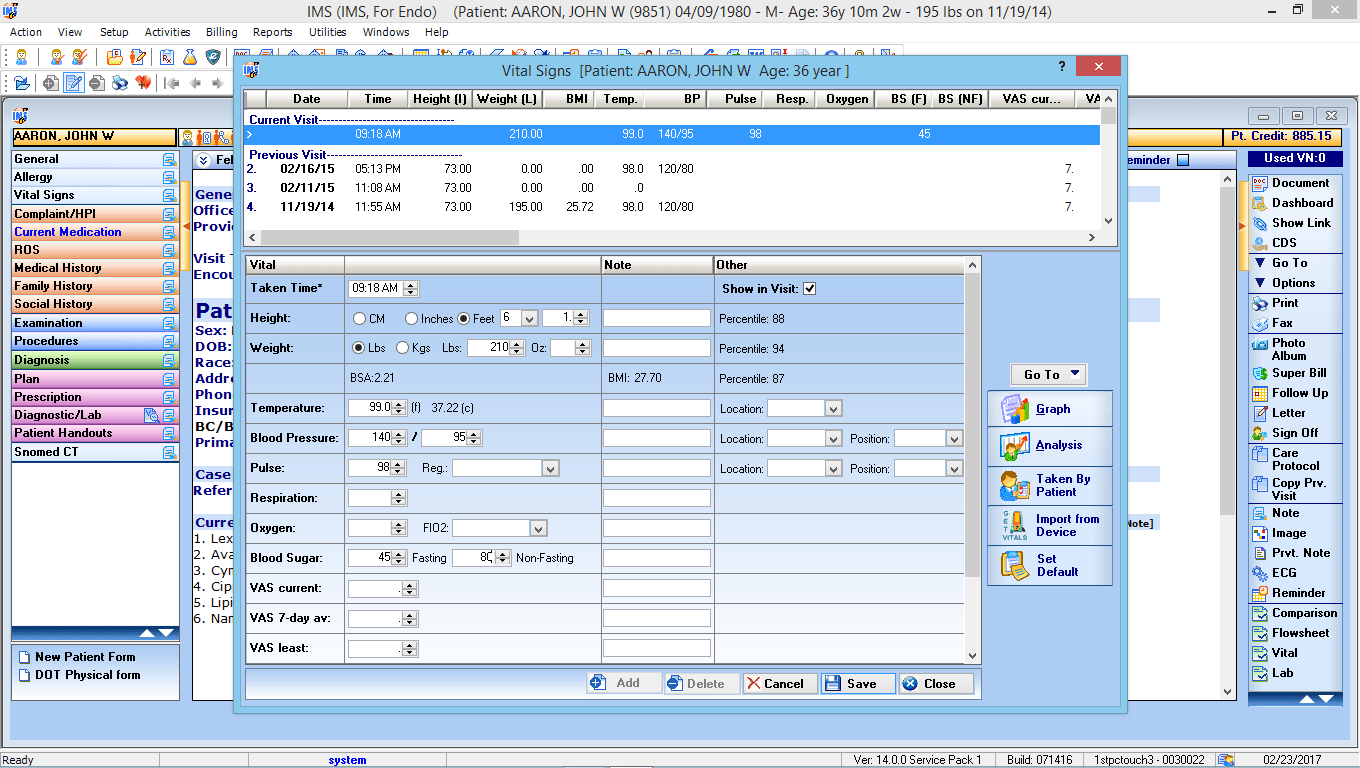
Vitals Interface
With IMS, patient vitals can be transferred wirelessly from your vitals device to the EMR. Vitals auto-populate in the patient’s chart, eliminating data entry and reducing errors.
Benefits
- Facilitates efficient data transfer
- Meets HIPAA standards
- Compliant with HL7, CCD, CCR
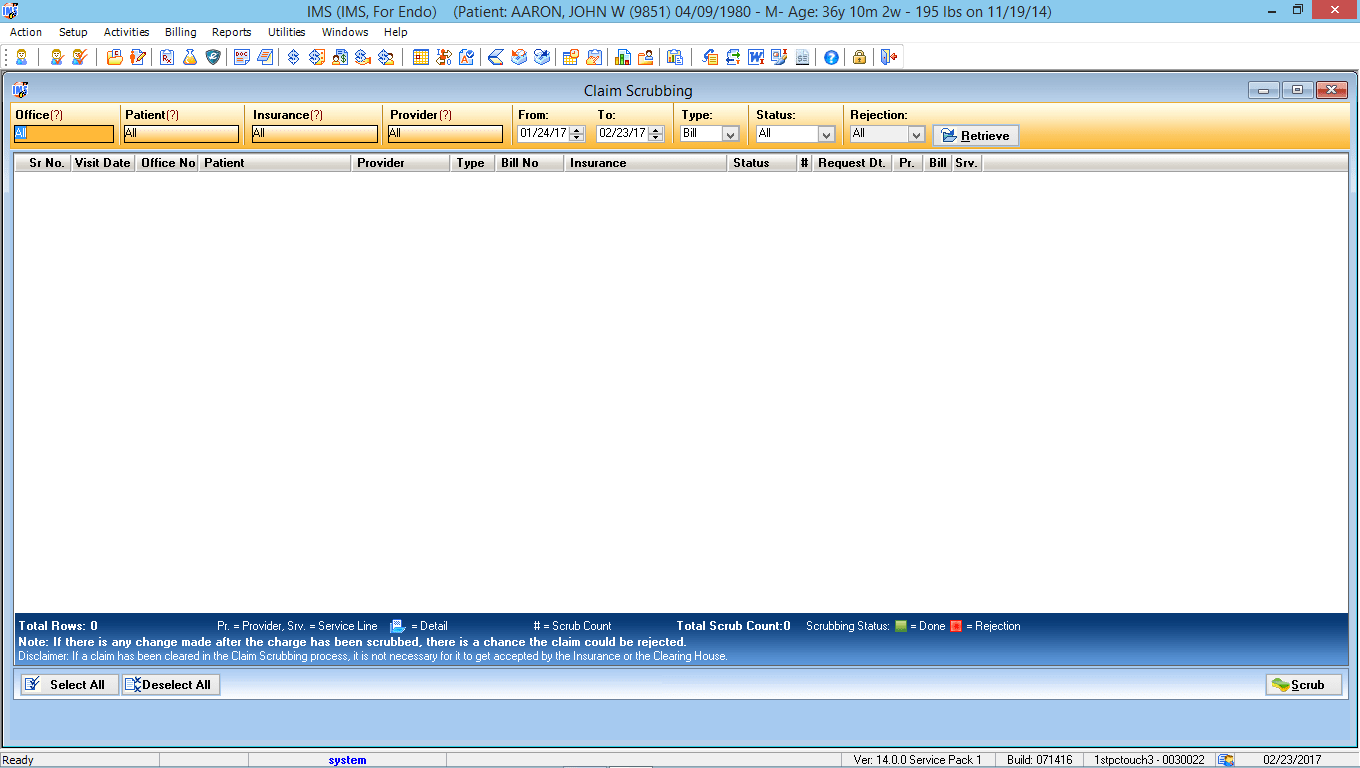
Advanced Clinical Editor
IMS’ advanced claims scrubbing technology allows Endocrinology specialists to check for claim errors in real-time, eliminate denials, and expedite the payment process.
Benefits
- Submit clean claims the first time
- Avoid processing delays
- Reduce denials
- Streamline workflow
Electronic Patient Statements
Transmit patient statements electronically and resolve collection issues more efficiently with our automated statement processing service.
Benefits
- Increase efficiency
- Reduce accounts receivable
- Eliminate forms and paper-based costs

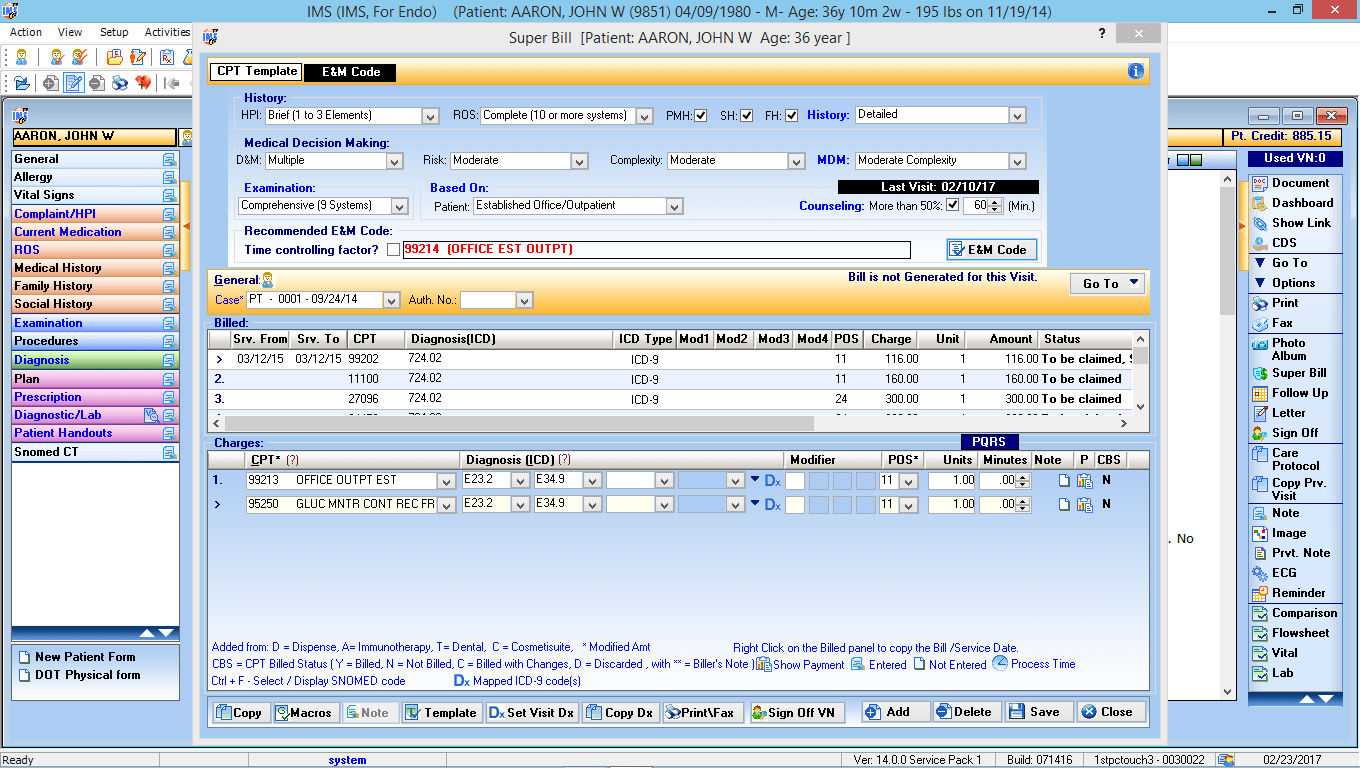
Electronic Super Bill
Create electronic super bills directly from your Endocrinology EMR for quick and simplified charge entry. You can even customize the super bills to meet the needs of each provider in your practice.
Benefits
- Capture all charges from your patient visits
- Reduce paper expenses
- Eliminate lost or missing forms

Revenue Cycle Management
Streamline office functions, see fewer missed payments, and help your Endocrinology practice run more efficiently than ever with IMS’ Revenue Cycle Management software.
Benefits
- Automate data entry
- Maximize revenue
- Increase productivity

CPT Code Advisor
IMS’ CPT Coding Advisor will review factors such as HPI and time spent with the patient and recommend appropriate E&M codes to ensure that payer documentation needs are adequately met.
Benefits
- Pre-screen claims automatically
- Check authorization requirements
- Reduce denials
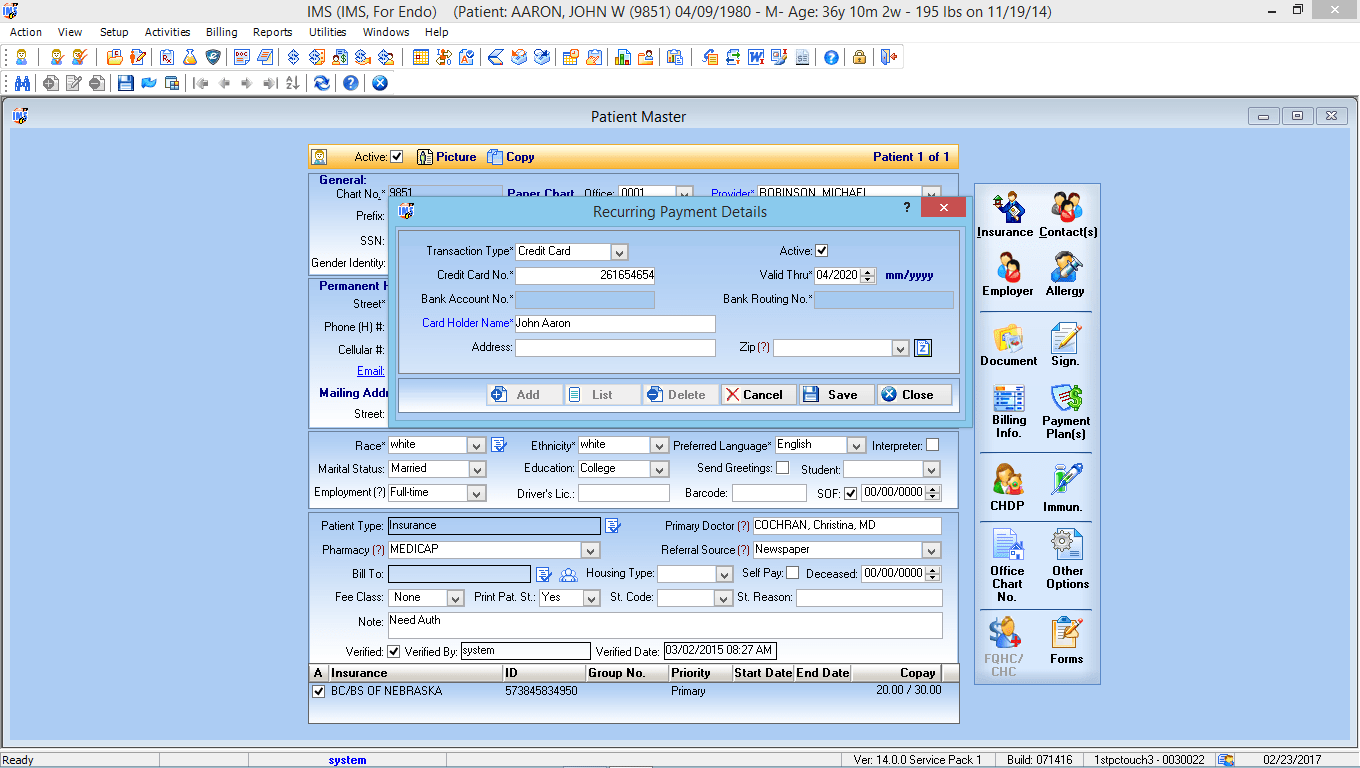
Patient Payment Solutions
Our EMR-integrated patient payment solution allows providers to collect payments from patients in person, online securely, and over the phone.
Benefits
- Provide multiple payment options
- Increase revenue
- Improve patient satisfaction
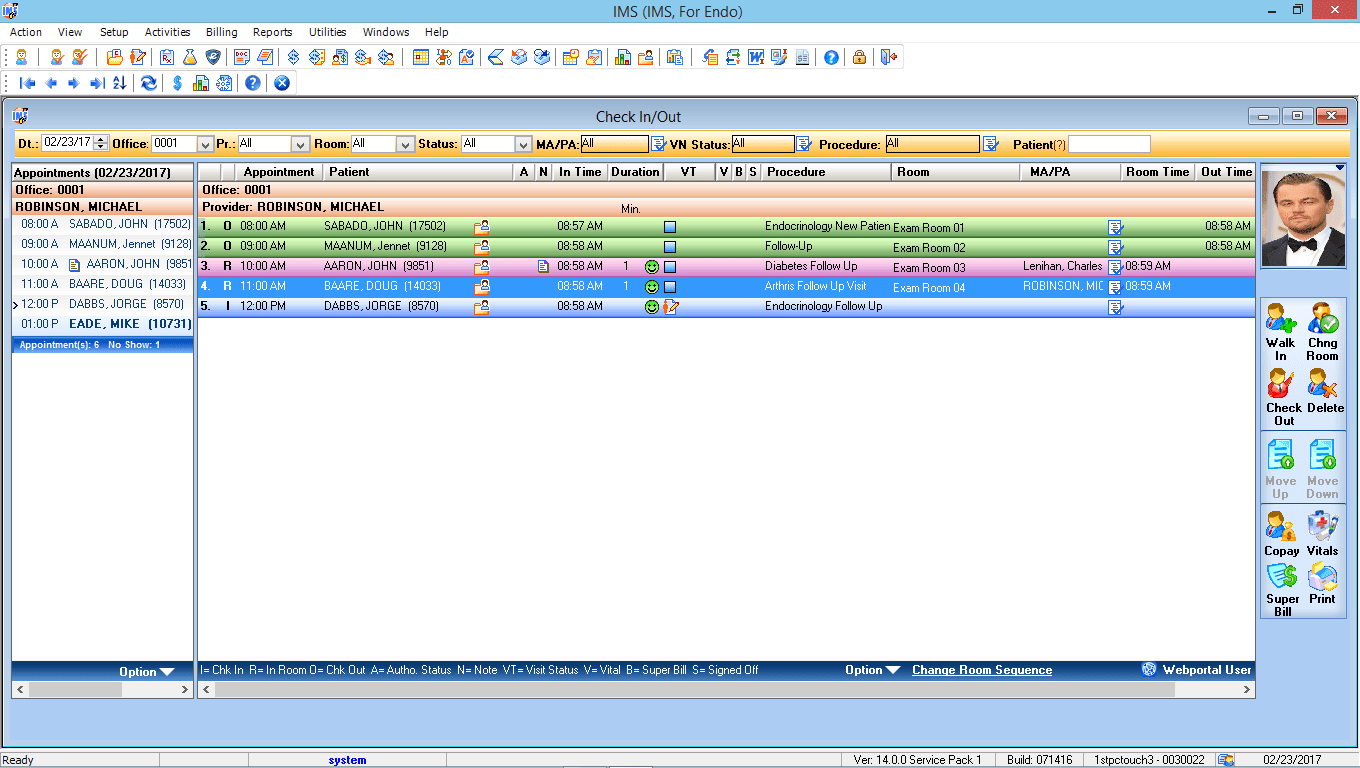
Check-In/Check-Out
IMS’ check-in/check-out feature allows staff to manage patients as they move about the office during their visit. It starts with the initial intake and ends at check out.
Benefits
- Keep track of patients
- Improve intra-office communication
- Effectively manage office resources
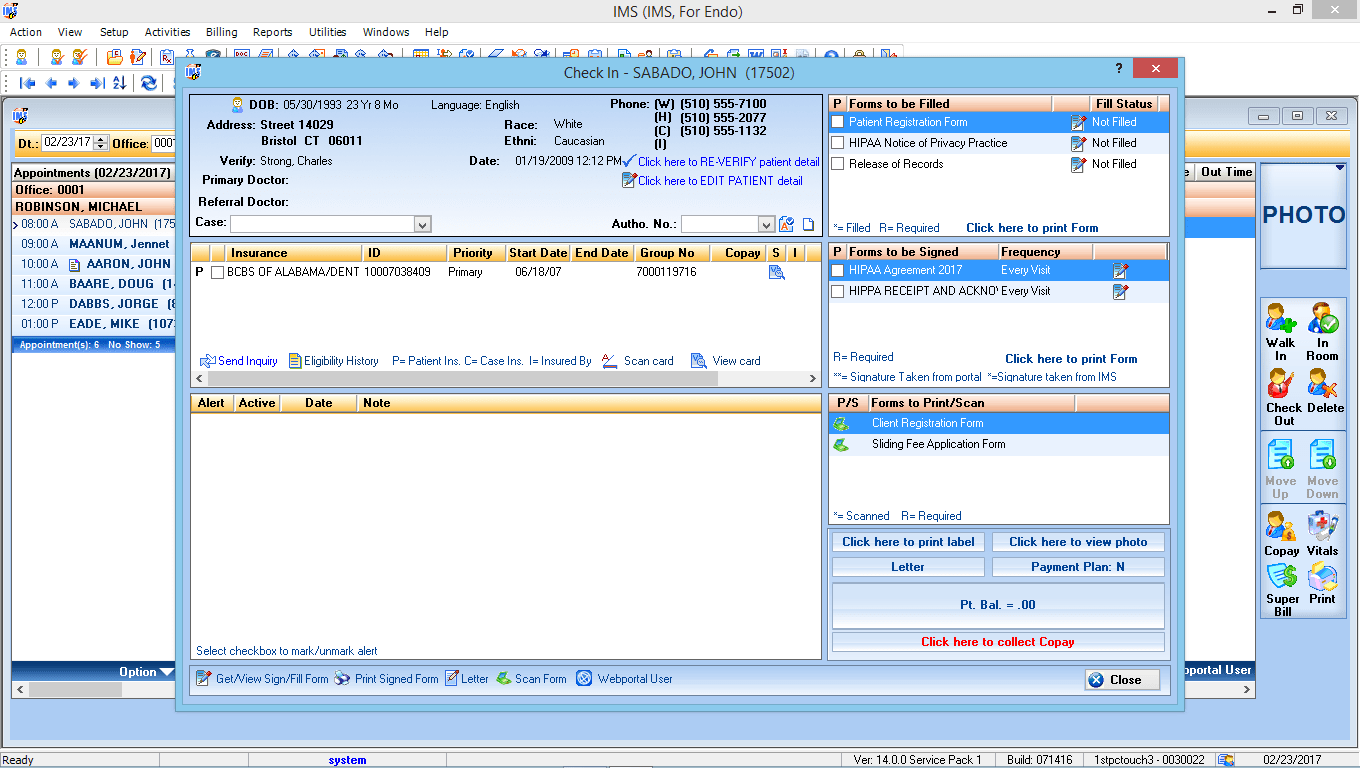
Check-In
Achieve a truly paperless environment with IMS’ patient check-in module. It covers all aspects of the intake process, from updating patient data to collecting co-pays or co-insurances.
Benefits
- Achieve maximum efficiency
- Streamline workflow
- Reduce check-in time
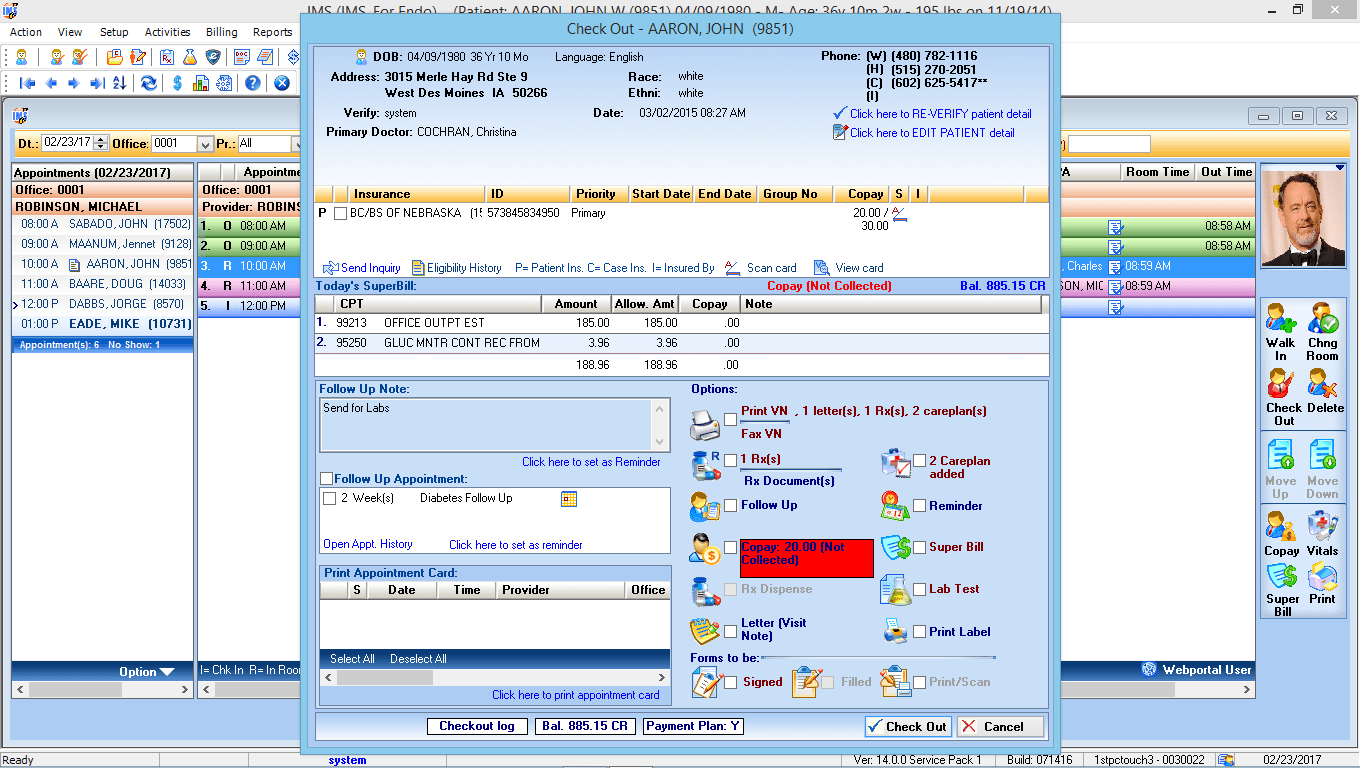
Check-Out
Ensure that all pending items are resolved before patients leave your office. Our check-out feature will prompt you to schedule follow-up appointments, collect patient responsibility, and more.
Benefits
- Increase collections
- Make better use of staff resources
- Improve patient satisfaction
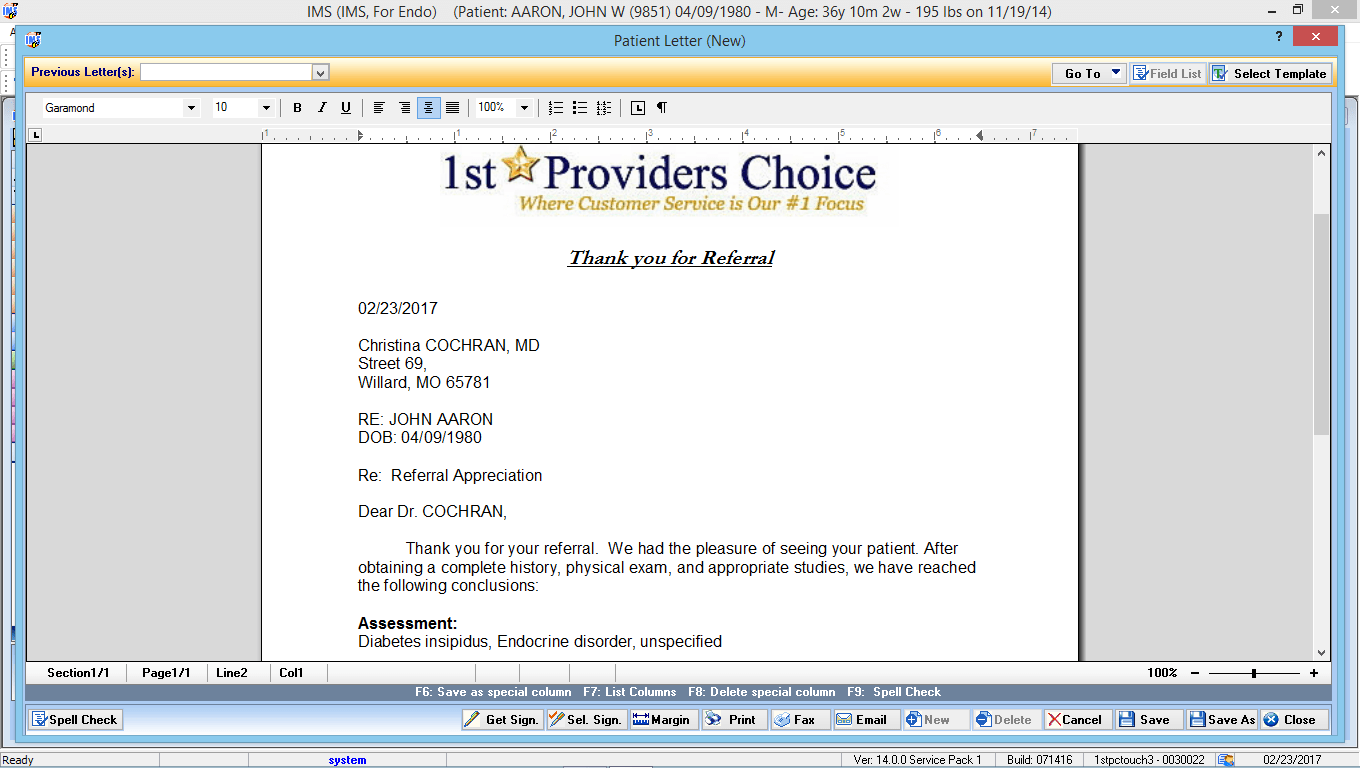
Letters/Forms Automation
IMS EMR features Endocrinology-specific forms and letters that providers in your field use most. You also have the option of generating custom documents with the input fields of your choice.
Benefits
- Eliminate paper forms
- Save time
- Improve productivity
Patient Appointment Scheduling
With an intuitive, customizable appointment scheduler, doctors and staff can easily manage patient appointments – including schedules for multiple offices and providers.
Benefits
- Reduce missed appointments
- Improve office productivity
- Eliminate overbookings

Patient Check-In Kiosk
Save time and money by allowing patients to check-in, update demographics, provide an electronic signature, and more at an easy-to-use check-in kiosk.
Benefits
- Streamline patient registration
- Reduce waiting time at check-in
- Use staff resources more efficiently

Patient Phone Reminders
IMS’ Interactive Voice Reminders service integrates with the appointment scheduling software to ensure that all of your patients receive reminders about their upcoming appointments.
Benefits
- Use live-person and automated reminders
- Decrease missed appointments
- Increase productivity
- Improve patient satisfaction

Authorization Tracking
IMS’ powerful Authorization Tracking module will help your Endocrinology practice track and manage all patient authorizations from one place in your EMR.
Benefits
- Pre-validate procedures quickly and easily
- Make better use of staff resources
- Improve productivity
Eligibility Tracking
Determine the status of your patient’s insurance coverage before the date of service with IMS’ eligibility verification module.
Benefits
- Reduce rejected claims
- Save staff time
- Increase revenue
- Improve patient relationships
Fax Integration
With IMS’ integrated fax module, Endocrinology specialists can send faxed documents directly into patients’ charts without scanning and fax patient data from the EMR.
Benefits
- Reduce paper and printing costs
- Improve productivity
- Maximize efficiencies
- Enhance workflows

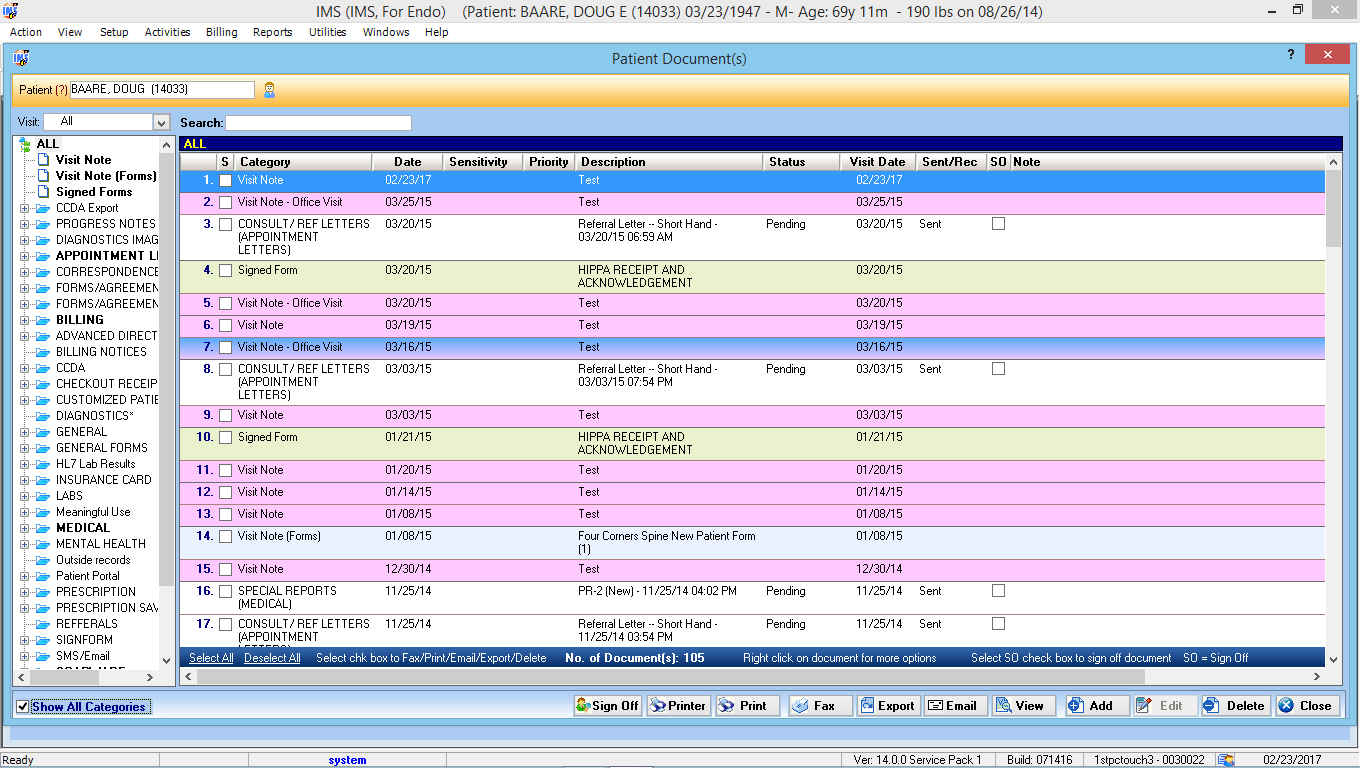
Patient Documents
Create a custom list of folders and subfolders to manage documents stored in each of your patients’ charts. Documents can then be faxed or emailed directly from the EMR.
Benefits
- Organize documents more efficiently
- Easily find pertinent information
- Increase productivity
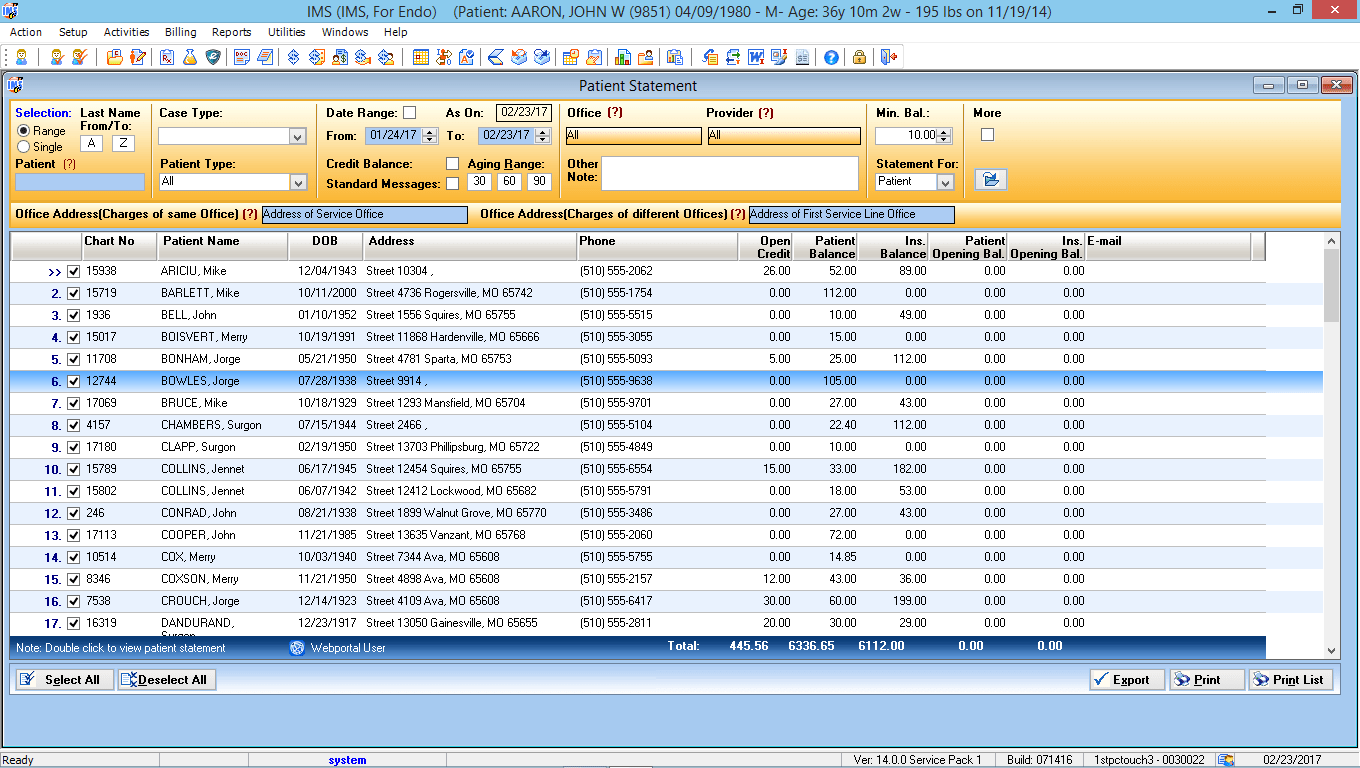
Patient Statement Preview List
Preview patient statements in an easy-to-navigate format and schedule statements to send out on a weekly or biweekly basis.
Benefits
- Improve productivity
- Increase practice revenue
- Maximize efficiency
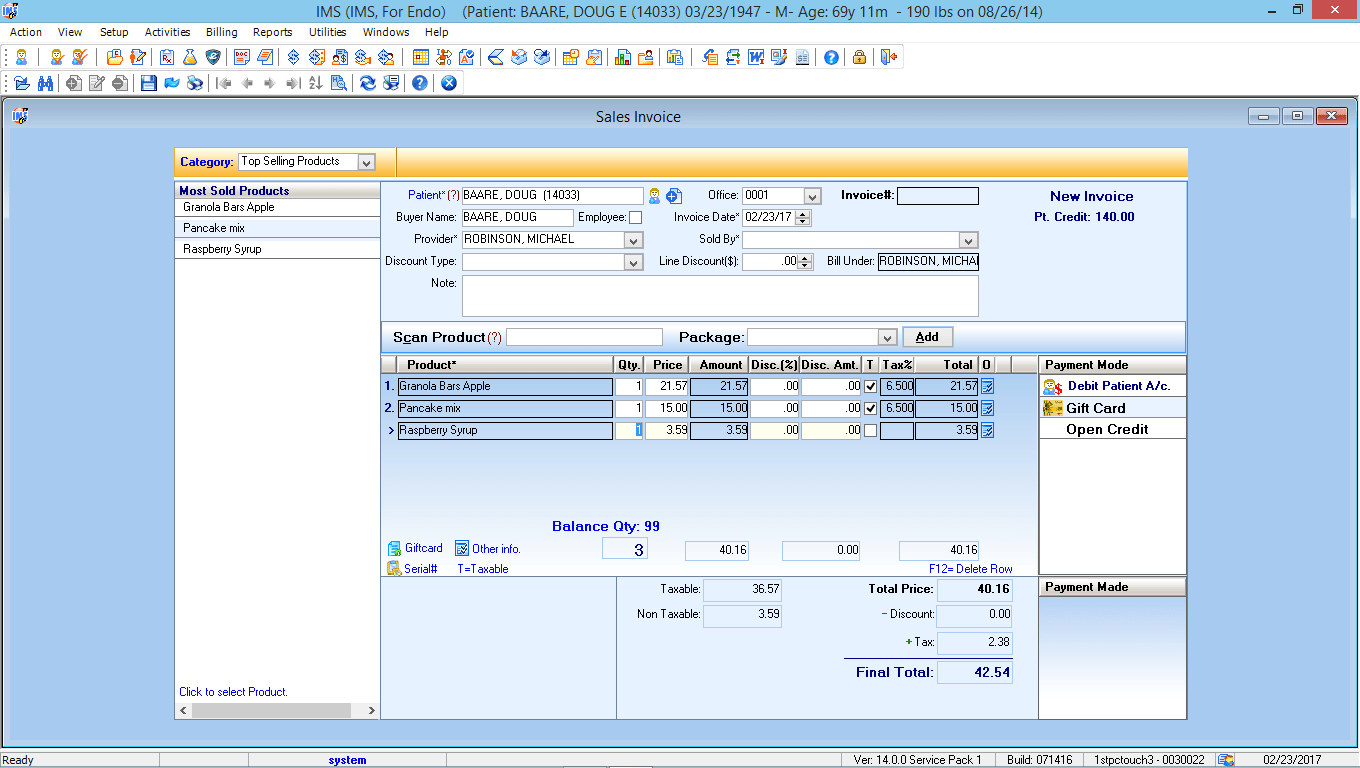
Point of Sales Module
From bar code scanning to inventory management, IMS’ point of sale capabilities will allow you to run a more efficient practice by ensuring you have the right supplies on hand at all times.
Benefits
- Streamline the check-out process
- Increase profits
- Maximize efficiency
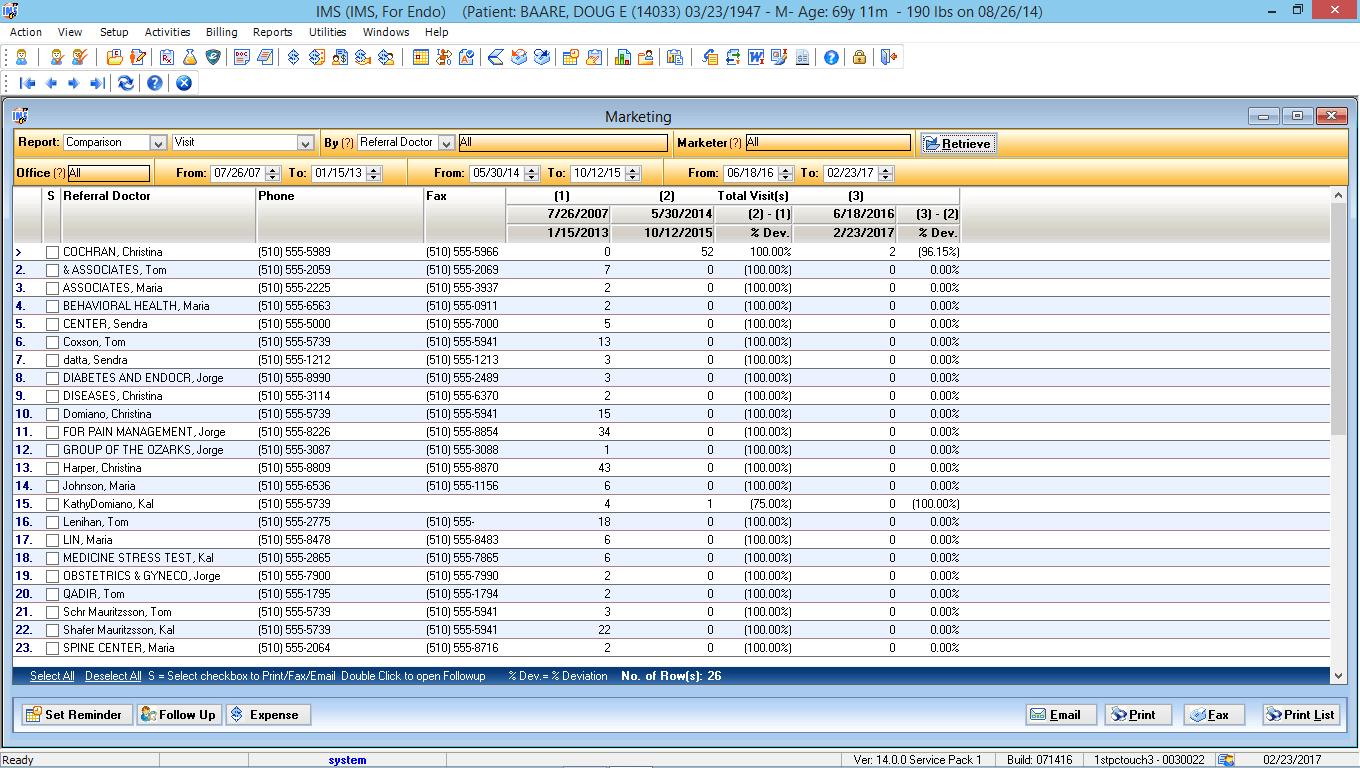
Marketing Module
Help make marketing decisions, track marketing expenses, and take advantage of custom reporting capabilities with our EMR-integrated marketing module.
Benefits
- Manage and organize leads
- Increase revenue
- Improve patient recall and retention
Health Maintenance Tracking
Keep track of patients’ health with IMS’ health maintenance tracking feature. Physicians receive alerts when things are due when patients need a follow-up call, when lab results are in, and more.
Benefits
- Improve patient health
- Provide better care quality
- Increase patient satisfaction
- Improve practice efficiencies
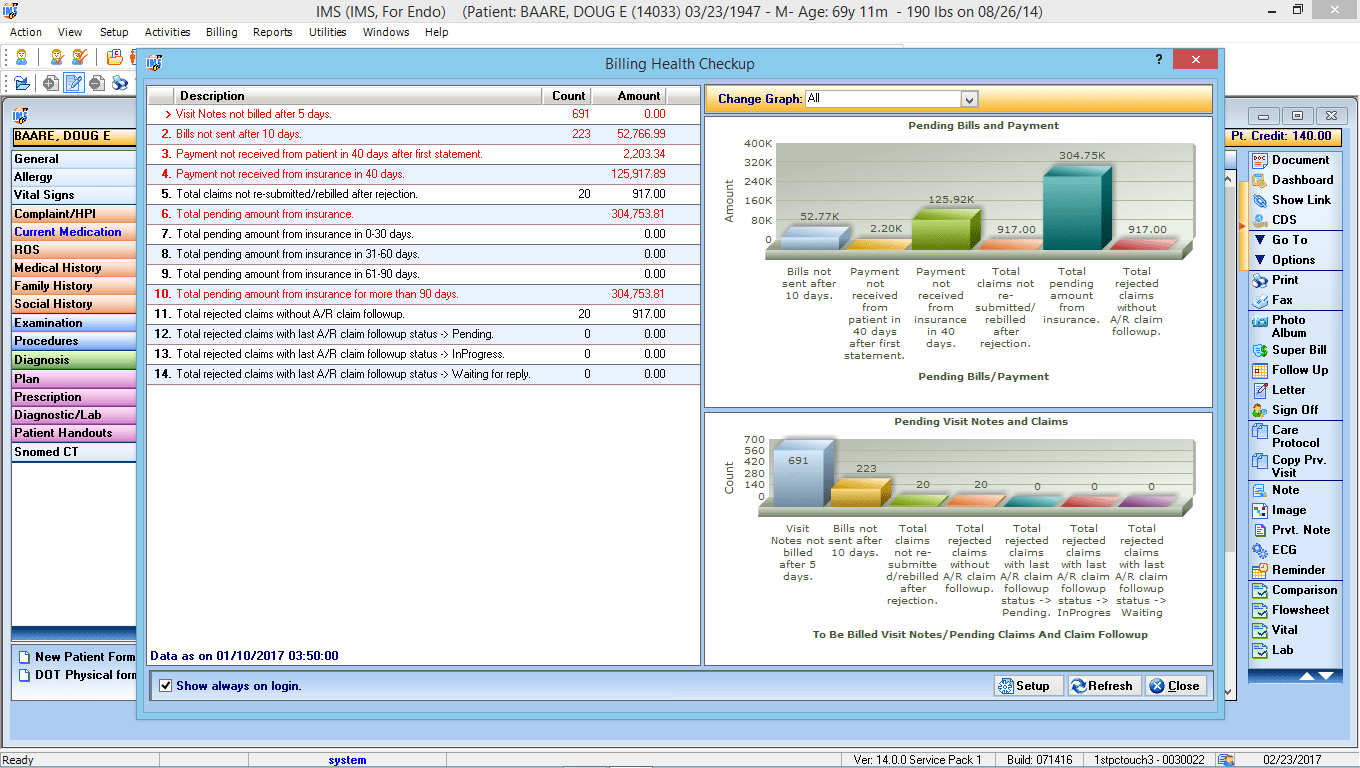
EMR & Billing Reporting Graphs
Find out how your practice is doing by running billing reports and graphs with a click of a button. The provider can generate graphs, insurance carrier, procedure, referring provider, and more.
Benefits
- Monitor your practice’s finances
- Increase collections